ERP evaluation of EEG signals for monitoring anesthesia depth during surgery
DOI:
https://doi.org/10.15419/bmrat.v10i10.841Keywords:
Anesthesia, Bi spectral analysis, EEG, AEP, ERP, Auditory nerve stimulationAbstract
Background: In medicine, general anesthesia during surgery involves the administration of pharmacological (hypnotic) agents and clinical monitoring via the analysis of the patient's nervous systems (loss of consciousness and reactivity) during stimulation. Unfortunately, this clinical monitoring is complicated by factors such as curarization, shock, and drugs that block cardiovascular responsiveness. Additionally, inadequate anesthesia due to over- or underdosing increases morbidity rates, such as hypotension and respiratory depression in the case of overdose, and memorization, movement, hypertension, tachycardia, laryngospasm, and bronchospasm in the case of underdosing. Several anesthesia monitoring tools have been introduced to address this issue, such as bispectral analysis (BIS), auditory evoked potential (AEP), q-CON, and entropy monitors; however, these instruments are complicated by accuracy, noise, artifacts, and their correlation with hypnotics.
Methods: Noninvasive anesthesia monitoring methods include lower esophageal sphincter, AEP, entropy, and spontaneous electroencephalography (EEG), which is the most commonly used. This method involves BIS of the collected EEG signals and correlates well with consciousness and sedation scores regardless of the anesthetic agents used. In this paper, we present a noninvasive method for monitoring the depth of anesthesia during surgery using the AEP and BIS methods. This study aimed to reduce artifacts, optimize the hypnotics/analgesics dosage, limit the effects of pharmacological use, and ensure a better quality recovery.
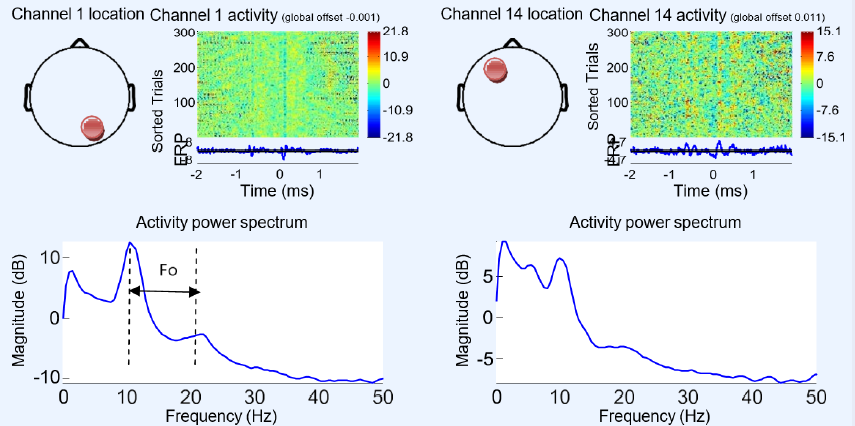
Results: We applied two techniques, BIS and event-related potential (ERP), following multiple stimuli to determine the best anesthesia monitoring approach. A comparative study of the EEG signals showed that measuring cortical responses by ERP provided more precise data in space and time regarding the sedation state of the patient and better monitoring of the hypnotic dose. The BIS method was simpler and easier to implement; however, only average and static values regarding the sleep rate could be obtained.
Conclusion: BIS and ERP appear suitable for monitoring sedation and hypnotic dosage during anesthesia, with the best reliability rates and speed with a latency of < 4 ms and an accuracy of 92%.
Published
Issue
Section
License
Copyright The Author(s) 2017. This article is published with open access by BioMedPress. This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.